Instructive Surfaces for Fibroblast Responses

Current Students
Anuraag Boddupalli, Chemical & Biological Engineering Ph.D. student
Zihao Xu, Materials Science & Engineering Ph.D. student
References
-
1.B. D. Ratner, A. S. Hoffman, F. J. Schoen, J. E. Lemons, Biomaterials Science: An Introduction to Materials in Medicine, Elsevier Academic Press, London 2004.
-
2.M. M. Stevens, J. H. George. Exploring and engineering the cell surface interface. Science, 2005, 310, 1135-1138.
-
3.A. G. Gristina. Biomaterial-centered infection: Microbial adhesion versus tissue integration. Science, 1987, 237, 1588-1595.
-
4.J. S. Boateng, K. H. Matthews, H. N. E. Stevens, G. M. Eccleston. Wound healing dressings and drug delivery systems: A review. Journal of Pharmaceutical Sciences, 2008, 97, 2892-2923.
-
5.J. M. Anderson, A. Rodriguez, D. T. Chang. Foreign body reactions to biomaterials. Seminars in Immunology, 2008, 20, 86-100.
-
6.J. M. Anderson, M. S. Shive. Biodegradation and biocompatibility of PLA and PLGA microspheres. Advanced Drug Delivery. 1997, 28, 5-24.
-
7.B. Rihova. Immunocompatibility and biocompatibility of cell delivery systems. Advanced Drug Delivery Reviews, 2000, 42, 65-80.
Overview
Approximately 100,000 skin grafts are performed annually. (“Georgia Health Sciences University/Tissue Donor Services” 2010) Typically, these grafts are used to treat acute injuries, burns, and chronic wounds. Emblematic risks associated with grafts include infection, rejection, loss of grafted skin, and bleeding.[1] Many of the problems associated with skin grafts may be solved through the use of polymeric gels formed in situ that augment the healing process while mitigating infection.
Polymers influence cell adhesion, proliferation, and morphology.[2,3] Wound-healing polymers must attain rapid healing with minimal scarring and disruption to the patient.[4] Therefore, our long-term goal is to rationally design rapidly curing wound-healing systems.
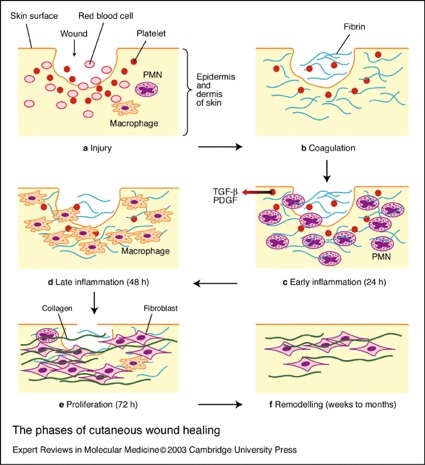
Immunological responses are dynamic processes and, as such, cell type and population at the implant site change during the healing process.[5] The sequence of local events following implantation is generally regarded as the tissue response continuum in which each individual event leads to the subsequent: injury progresses to acute inflammation, which proceeds to chronic inflammation, followed by granulation tissue formation, foreign body reaction and fibrous encapsulation.[5,6] The presence of eosinophils and polymorphonuclear (PMN) cells typify acute inflammatory responses while macrophages and fibroblasts signify the chronic form.[7]
Approaches
We employ in vivo imaging methods to visualize both phagocytic and fibrotic wound-healing responses. The tissue response to implanted materials as a function of time will improve fundamental knowledge in wound-healing responses, as well as enhance rational design for wound-healing systems. We synthesize novel polymers that alter the response of fibroblasts and we assess the molecular response of cells to the polymers in vitro.
The Bratlie Research Group
Department of Materials Science and Engineering
Department of Chemical and Biological Engineering
Iowa State University, Ames, IA 50011
© 2011 Kaitlin Bratlie

